Quantum breakthrough could revolutionize computing
Pallab Ghosh – Science correspondent – February 8, 2023
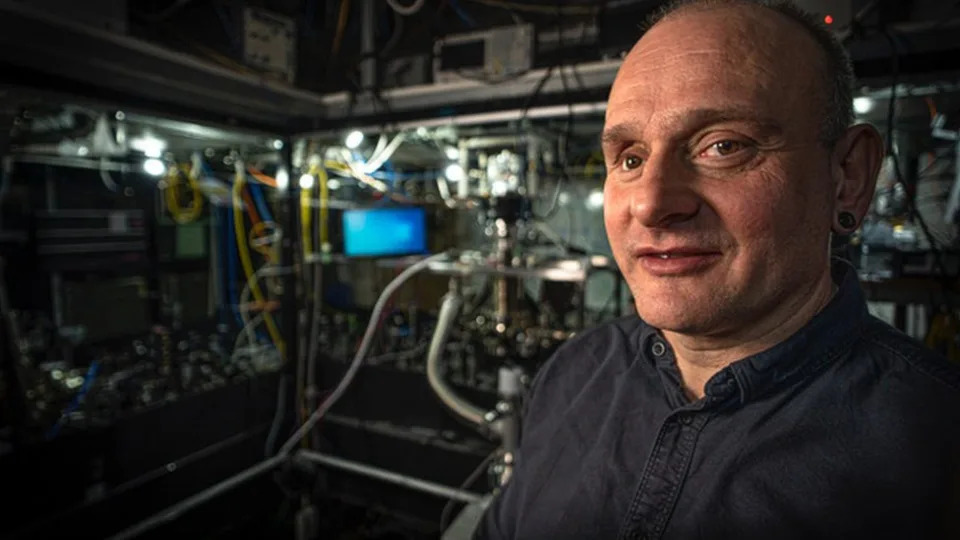
Twenty years ago Winfried Hensinger was told by other scientists that developing a powerful quantum computer was impossible. Now he has made the system behind him that he believes will prove them wrong
Scientists have come a step closer to making multi-tasking ‘quantum’ computers, far more powerful than even today’s most advanced supercomputers.
Quantum computers make use of the weird qualities of sub-atomic particles.
So-called quantum particles can be in two places at the same time and also strangely connected even though they are millions of miles apart.
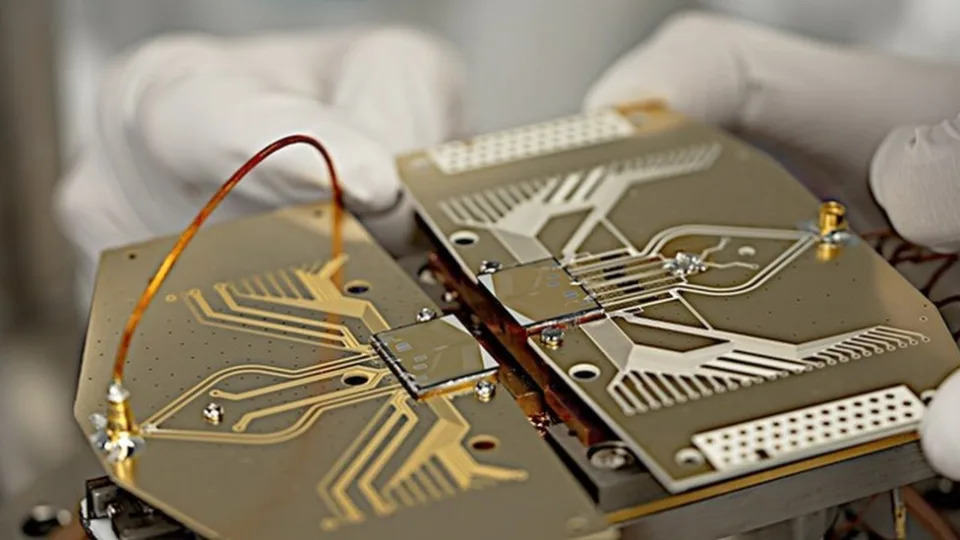
A Sussex University team transferred quantum information between computer chips at record speeds and accuracy.
The researchers connected two chips together and sent record amounts of quantum information at unprecedented speeds and reliability
Computer scientists have been trying to make an effective quantum computer for more than 20 years. Firms such as Google, IBM and Microsoft have developed simple machines. But, according to Prof Winfried Hensinger, who led the research at Sussex University, the new development paves the way for systems that can solve complex real world problems that the best computers we have today are incapable of.
“Right now we have quantum computers with very simple microchips,” he said. “What we have achieved here is the ability to realise extremely powerful quantum computers capable of solving some of the most important problems for industries and society.”
Rolls-Royce is investing in quantum computing research to see if it can speed up the design process for their aircraft engines
Currently, computers solve problems in a simple linear way, one calculation at a time.
In the quantum realm, particles can be in two places at the same time and researchers want to harness this property to develop computers that can do multiple calculations all at the same time.
Quantum particles can also be millions of miles apart and be strangely connected, mirroring each other’s actions instantaneously. Again, that could also be used to develop much more powerful computers.
The quantum computer chips have to be set up in a clean room an put into a vacuum container as even the slightest contamination can reduce its performance
One stumbling block has been the need to transfer quantum information between chips quickly and reliably: the information degrades, and errors are introduced.
But Prof Hensinger’s team has made a breakthrough, published in the journal Nature Communications, which may have overcome that obstacle.
The team developed a system able to transport information from one chip to another with a reliability of 99.999993% at record speeds. That, say the researchers, shows that in principle chips could be slotted together to make a more powerful quantum computer.
The research team can see individual atoms floating above their chips as the test out their quantum computer
Prof Michael Cuthbert, who is the director of the newly established National Quantum Computing Centre in Didcot, Oxfordshire and is independent of the Sussex research group described the development as a “really important enabling step”. But he said that more work was needed to develop practical systems.
“To build the type of quantum computer you need in the future, you start off by connecting chips that are the size of your thumbnail until you get something the size of a dinner plate. The Sussex group has shown you can have the stability and speed for that step.
“But then you need a mechanism to connect these dinner plates together to scale up a machine, potentially as large as a football pitch, in order to carry out realistic and useful computations, and the technology for communications for that scale is not yet available.”
Quantum computers harness two weird properties of particles at the very small scale – they can be in two places at the same time and be strangely connected even though they are millions of miles apart.
PhD student Sahra Kulmiya, who carried out the Sussex experiment, says that the team are ready for the challenge to take the technology to the next level.
“It is not just solely a physics problem anymore,” she told BBC News.
“It is an engineering problem, a computer science problem and also a mathematical problem.
“It is really difficult to say how close we are to the realisation of quantum computing, but I’m optimistic in how it can become relevant to us in our everyday lives.”
One of the UK’s leading engineering firms, Rolls Royce, is also optimistic about the technology. It is working with the Sussex researchers to develop machines that could help them design even better jet engines.
Powerful supercomputers are used to model the flow of air in simulations to test out new designs of aircraft engines.
Transforming engineering
A quantum computer could in principle track the airflow with even greater accuracy, and do so really quickly, according to Prof Leigh Lapworth, who is leading the development of quantum computing for Rolls-Royce.
“Quantum computers would be able to do calculations that we can’t currently do and others that would take many months or years. The potential of doing those in days would just transform our design systems and lead to even better engines.”
The technology could potentially also be used to design drugs more quickly by accurately simulating their chemical reactions, a calculation too difficult for current supercomputers. They could also provide even more accurate systems to forecast weather and project the impact of climate change.
Prof Hensinger said he first had the idea of developing a quantum computer more than 20 years ago.
“People rolled their eyes and said: ‘it’s impossible’.”
“And when people tell me something can’t be done, I just love to try. So I have spent the past 20 years removing the barriers one by one to a point where one can now really build a practical quantum computer.”
Worried about having a gas stove? Here’s how to limit risks.
Allyson Chiu, The Washington Post – February 7, 2023
Note: This article has been updated to include additional safety information about using induction hot plates.
The raging gas stove debate might have you reassessing how you cook. But replacing a gas stove with an induction stove – a commonly recommended alternative – isn’t always feasible.
Renters are often limited in what they can do. For homeowners, swapping out a gas range can be expensive and complicated, especially if it involves electrical updates.
Still, even if you cannot get rid of your gas stove, you can take several steps to help protect your health and the planet:
Get reacquainted with your other appliances
A whole world of versatile and convenient cooking devices exist outside of your gas stove.
“There’s a lot of appliances available that can address different things you might need to do in the kitchen, and so you can go a long way toward electrifying all of your cooking,” said Talor Gruenwald, a research associate at Rewiring America, a nonprofit group focused on electrification.
Beyond the trusty microwave, you might have one or more of the following appliances taking up space in your kitchen: toaster oven, air fryer, Instant Pot (or some other multicooker), or an electric kettle or hot water heater.
Using them more, particularly for smaller meals, can help reduce the amount of pollutants, such as nitrogen dioxide, released into your home when you turn on your gas burners. Research has linked nitrogen dioxide to increased risk of childhood asthma and worsening asthma symptoms. A recent peer-reviewed study estimated that about 12.7 percent of childhood asthma cases nationwide could be attributed to gas cooking.
Here are some creative ways you can use your appliances:
– Microwaves: They can do much more than just zap cold leftovers. You can bake (remember mug cakes?), steam vegetables and in some situations even toast, fry or caramelize food. For more detailed tips on how you can make the most out of your microwave, read this article from my colleague Becky Krystal.
– Toaster ovens: Reheating leftovers, such as pizza or fries, that you don’t want to eat soggy? Broiling seafood, vegetables or a cheesy open-face sandwich? Baking savory casseroles or sweet desserts? Most modern toaster oven models can likely do it all. Read more here.
– Air fryers: You can make entire balanced and healthy meals in an air fryer in less than 30 minutes with inexpensive ingredients and minimal cleanup afterward, as my colleague Anahad O’Connor writes. You can also bake in air fryers.
– Instant Pots or multicookers: Aside from its handy pressure cooker feature, they can serve as effective steamers and slow cookers, and are even “equipped with a sauté or sear function, meaning you can use them as you would a pot or skillet on a traditional stovetop,” Krystal writes.
Pay attention to ventilation
If you do need to use your gas stove or oven, it can help to turn on your range hood while cooking, Gruenwald said.
Brady Seals, a manager in the carbon-free buildings program at RMI, a clean-energy think tank, recommends using the rear burners on your stovetop where the range hood can be more effective.
If your hood isn’t vented outside or you don’t have one, you should open your windows, experts said.
“You just want to try to move air and bring in clean air,” Seals said, noting that people can try turning on a bathroom fan. “Even opening a window for five minutes can sometimes be helpful in removing some of the pollutants.”
And don’t forget to maintain your gas stove. Some research has found that unused stoves can still leak methane, a powerful greenhouse gas, as well as other hazardous air pollutants, such as benzene. If you’re concerned about leaks, consider having a professional examine the fittings on your stove, Gruenwald said.
Experiment with induction
You can also buy a low-cost induction hot plate that plugs in to a regular outlet. Models are available with single or double burners.
What’s more, experts say you can turn your gas stove into a makeshift induction cooktop by first closing the gas valve behind the stove and then placing an electric hot plate on top. Make sure to double check that no gas is coming out of your burners and that all the knobs are also turned off. It may be helpful to use a butcher block or other sturdy flat surface to provide a firm footing for the hot plate.
“If you are curious about induction but aren’t able to make the switch because you’re a renter or other reasons, it’s a good way to try out the speed and see all the other benefits,” Seals said.
Huge chunk of plants, animals in U.S. at risk of extinction -report
Brad Brooks – February 6, 2023
A Venus flytrap is seen at the meat-eating plant exhibition “Dejate Atrapar” (Let Yourself Get Caught), in BogotaEndangered Key Deer are pictured in a puddle following Hurricane Irma in Big Pine Key, FloridaEndangered Arizona hedgehog cactus is seen in the Oak Flat recreation area outside Superior, ArizonaA full moon rises over a cactus in PhoenixThe endangered dusky gopher frog, a darkly colored, moderately sized frog with warts covering its back and dusky spots on its belly, is shown in this handout photo
(Reuters) -A leading conservation research group found that 40% of animals and 34% of plants in the United States are at risk of extinction, while 41% of ecosystems are facing collapse.
Everything from crayfish and cacti to freshwater mussels and iconic American species such as the Venus flytrap are in danger of disappearing, a report released on Monday found.
NatureServe, which analyzes data from its network of over 1,000 scientists across the United States and Canada, said the report was its most comprehensive yet, synthesizing five decades’ worth of its own information on the health of animals, plants and ecosystems.
Importantly, the report pinpoints the areas in the United States where land is unprotected and where animals and plants are facing the most threats.
Sean O’Brien, president of NatureServe, said the conclusions of the report were “terrifying” and he hoped it would help lawmakers understand the urgency of passing protections, such as the Recovering America’s Wildlife Act that stalled out in Congress last year.
“If we want to maintain the panoply of biodiversity that we currently enjoy, we need to target the places where the biodiversity is most threatened,” O’Brien said. “This report allows us to do that.”
U.S. Representative Don Beyer, a Democrat who has proposed legislation to create a wildlife corridor system to rebuild threatened populations of fish, wildlife and plants, said NatureServe’s work would be critical to helping agencies identify what areas to prioritize and where to establish migration routes.
“The data reported by NatureServe is grim, a harrowing sign of the very real problems our wildlife and ecosystems are facing,” Beyer told Reuters. “I am thankful for their efforts, which will give a boost to efforts to protect biodiversity.”
HUMAN ENCROACHMENT
Among the species at risk of disappearing are icons like the carnivorous Venus flytrap, which is only found in the wild in a few counties of North and South Carolina.
Nearly half of all cacti species are at risk of extinction, while 200 species of trees, including a maple-leaf oak found in Arkansas, are also at risk of disappearing. Among ecosystems, America’s expansive temperate and boreal grasslands are among the most imperiled, with over half of 78 grassland types at risk of a range-wide collapse.
The threats against plants, animals and ecosystems are varied, the report found, but include “habitat degradation and land conversion, invasive species, damming and polluting of rivers, and climate change.”
California, Texas and the southeastern United States are where the highest percentages of plants, animals and ecosystems are at risk, the report found.
Those areas are both the richest in terms of biodiversity in the country, but also where population growth has boomed in recent decades, and where human encroachment on nature has been harshest, said Wesley Knapp, the chief botanist at NatureServe.
Knapp highlighted the threats facing plants, which typically get less conservation funding than animals. There are nearly 1,250 plants in NatureServe’s “critically imperiled” category, the final stage before extinction, meaning that conservationists have to decide where to spend scant funds even among the most vulnerable species to prevent extinctions.
“Which means a lot of plants are not going to get conservation attention. We’re almost in triage mode trying to keep our natural systems in place,” Knapp said.
‘NATURE SAVINGS ACCOUNT’
Vivian Negron-Ortiz, the president of the Botanical Society of America and a botanist with the U.S. Fish and Wildlife Service, who was not involved in the NatureServe report, said there is still a lot scientists do not know and have not yet discovered about biodiversity in the United States, and that NatureServe’s data helped illuminate that darkness.
More than anything, she sees the new data as a call to action.
“This report shows the need for the public to help prevent the disappearance of many of our plant species,” she said. “The public can help by finding and engaging with local organizations that are actively working to protect wild places and conserve rare species.”
John Kanter, the senior wildlife biologist with the National Wildlife Federation, said the data in the report, which he was not involved with, was essential to guiding state and regional officials in creating impactful State Wildlife Action Plans (SWAPs), which they must do every 10 years to receive federal funding to protect vulnerable species.
Currently $50 million in federal funding is divided up among all states to carry out their SWAPs. The Recovering America’s Wildlife Act, whose congressional sponsors say will be reintroduced soon, would have increased that to $1.4 billion, which would have a huge impact on the state’s abilities to protect animals and ecosystems, Kanter said, and the NatureServe report can act as roadmap for officials to best spend their money.
“Our biodiversity and its conservation is like a ‘nature savings account’ and if we don’t have this kind of accounting of what’s out there and how’s it doing, and what are the threats, there’s no way to prioritize action,” Kanter said. “This new report is critical for that.”
Read more:
GRAPHIC-The collapse of insects
Penguins offer varied clues to Antarctic climate change
ANALYSIS-U.N. nature deal can help wildlife as long as countries deliver
(Reporting by Brad Brooks in Lubbock, Texas; Additional reporting by Julio-Cesar Chavez in Washington; Editing by Lisa Shumaker)
Death toll climbs as 7.8 magnitude earthquake rocks Turkey and Syria: Here’s everything we know
Photos show the devastation and desperate search for survivors after an earthquake hit the border of Turkey and Syria.
Dylan Stableford and Yahoo News Photo Staff – February 6, 2023
Rescuers carry out a girl from a collapsed building following an earthquake in Diyarbakir, Turkey February 6, 2023. (Sertac Kayar/Reuters)
At least 2,300 people were killed after a 7.8 magnitude pre-dawn earthquake rocked the border of Turkey and Syria early Monday, toppling thousands of buildings and leaving hundreds of people trapped under rubble.
The quake, which was centered on Turkey’s southeastern province of Kahramanmaras, could be felt as far away as Cairo and Beirut, as powerful aftershocks continued to rattle the region.
Here’s everything we know about the earthquake and its aftermath.
This aerial view shows residents searching for victims and survivors amidst the rubble of collapsed buildings following an earthquake in the village of Besnia near the twon of Harim, in Syria’s rebel-held northwestern Idlib province on the border with Turkey, on February 6, 2022. (Omar Haj Kadour/AFP via Getty Images)
The U.S. Geological Survey measured the 7.8 magnitude quake at a depth of 17.9 km, or about 11 miles, at 4:17 a.m. local time.
“On both sides of the border, residents jolted out of sleep by the pre-dawn quake rushed outside on a cold, rainy and snowy night. Buildings were reduced to piles of pancaked floors,” the news service reported. “Rescue workers and residents in multiple cities searched for survivors, working through tangles of metal and concrete. A hospital in Turkey collapsed, and patients, including newborns, were evacuated from facilities in Syria.”
An infographic titled “Impact area of earthquakes in Turkey” created in Ankara, Turkiye on February 06, 2023. (Yasin Demirci/Anadolu Agency via Getty Images)
Dozens of aftershocks followed. Hours later, a 7.5 magnitude quake struck more than 60 miles away. An official from Turkey’s disaster management agency said it was a new earthquake, not an aftershock, the AP said.
Death toll climbs
In Turkey, officials said the death toll had risen to almost 1,500, with at least 8,500 injured.
In Syria, the death toll in government-held areas was at least 430 with more than 1,200 injured, the Syrian Health Ministry reported. In rebel-held areas, more than 380 people were killed, according to the Syrian Civil Defense unit, also known as the White Helmets.
Search and rescue operations continue after 7.7 magnitude earthquake hits Elazig, Turkiye on February 06, 2023. (Ismail Sen/Anadolu Agency via Getty Images)
Turkish President Recep Tayyip Erdogan warned that the death toll will undoubtedly rise.
“Because the debris removal efforts are continuing in many buildings in the earthquake zone, we do not know how high the number of dead and injured will rise,” Erdogan said. “Hopefully, we will leave these disastrous days behind us in unity and solidarity as a country and a nation.”
Winter weather complicates recovery efforts
Bitterly cold temperatures and worsening conditions were complicating the search and rescue efforts, Reuters reported.
Civil defense workers and security forces search through the wreckage of collapsed buildings in Hama, Syria, Monday, Feb. 6, 2023. (SANA via AP)
“Temperatures in some areas were expected to fall to near freezing overnight, worsening conditions for people trapped under rubble or left homeless,” the news service said. “Rain was falling on Monday after snowstorms swept the country at the weekend.”
What’s more, “poor internet connections and damaged roads between some of the worst-hit cities in Turkey’s south, homes to millions of people, hindered efforts to assess and address the impact.”
Quake struck war-torn region
The earthquake struck a region that has been battered on both sides of the border by more than a decade of civil war in Syria.
Rescue teams search for victims in the rubble following an earthquake in northwestern Syrian Idlib in the rebel-held part of Idlib province, on February 6, 2023. (Syria Civil Defense/UPI/Shutterstock)
“On the Syrian side, the region is divided between government-held territory and the country’s last opposition-held enclave, which is surrounded by Russian-backed government forces. Turkey is home to millions of refugees from that conflict. About 4 million people live in the opposition-held regions in Syria, many of them displaced from other parts of the country by the fighting. Many of the residential buildings were already unsafe because of bombardments.”
Mehmet Emin Ataoglu rescued under the rubble of 6-storey-building after 7.7 magnitude earthquake hits Iskenderun district of Hatay, Turkiye on February 06, 2023. (Murat Sengul/Anadolu Agency via Getty Images)
The region also sits on top of major fault lines. In 1999, a string of earthquakes struck northwest Turkey, killing nearly 18,000 people.
Erdogan called Monday’s quake the biggest disaster since the 1939 Erzincan earthquake, which killed more than 30,000.
Biden vows support
Civil defense workers and security forces search through the wreckage of collapsed buildings in Hama, Syria, Monday, Feb. 6, 2023. (Omar Sanadik/AP)
In a statement, President Biden said he was “deeply saddened by the loss of life and devastation caused by the earthquake” and has directed his administration to provide any and all needed assistance.
“Our teams are deploying quickly to begin to support Turkish search and rescue efforts and address the needs of those injured and displaced by the earthquake,” Biden said in a statement. “U.S.-supported humanitarian partners are also responding to the destruction in Syria. Today, our hearts and our deepest condolences are with all those who have lost precious loved ones, those who are injured, and those who saw their homes and businesses destroyed.”
More images from the devastation
Rescue teams evacuate a victim pulled out of the rubble following an earthquake in northwestern Syrian Idlib in the rebel-held part of Idlib province, on February 6, 2023. (Syria Civil Defense/UPI/Shutterstock)People gather as rescuers search for survivors under the rubble, following an earthquake, in rebel-held town of Jandaris, Syria February 6, 2023. (Khalil Ashawi/Reuters)A rescuer carries an injured child away from the rubble of a building following an earthquake in rebel-held Azaz, Syria February 6, 2023 in this still image taken from video. Reuters TV/via Reuters)Rescuers search for survivors under the rubble, following an earthquake, in rebel-held town of Jandaris, Syria February 6,2023. (Khalil Ashawi/Reuters)Firefighters carry the body of a victim in Diyarbakir, in southeastern Turkey, Monday, Feb. 6, 2023. (Mahmut Bozarsan/AP)Syrian civil defense members search for people under the rubble of a destroyed building in Afrin, Syria, Monday, Feb. 6, 2023. (Zana Halil/DIA images via AP)People and emergency teams rescue a person on a stretcher from a collapsed building in Adana, Turkey, Monday, Feb. 6, 2023. (IHA agency via AP)People search for survivors under the rubble following an earthquake in Diyarbakir, Turkey February 6, 2023. (Sertac Kayar/Reuters)People carry a victim as rescuers search for survivors under the rubble, following an earthquake, in rebel-held town of Jandaris, Syria February 6, 2023. (Khalil Ashawi/AP)Rescuers work at the site of a collapsed building following an earthquake in Adana, Turkey February 6, 2023. (Cagla Gurdogan/Reuters)A man carries a girl following an earthquake, in rebel-held town of Jandaris, Syria February 6, 2023. (Khalil Ashawi/Reuters)People gather as rescuers search for survivors under the rubble, following an earthquake, in rebel-held town of Jandaris, Syria February 6, 2023. (Khalil Ashawi/Reuters)Earthquake victims receive treatment at the al-Rahma Hospital in the town of Darkush, Idlib province, northern Syria, Monday, Feb. 6, 2023. (Ghaith Alsayed/AP)
EXPLAINER – Why was the Turkey-Syria earthquake so bad?
Gloria Dickie – February 6, 2023
Earthquake in IskenderunAftermath of an earthquake in Aleppo
LONDON (Reuters) – The magnitude 7.8 earthquake that struck Turkey and Syria on Monday is likely to be one of the deadliest this decade, seismologists said, with a more than 100 km (62 miles) rupture between the Anatolian and Arabian plates.
Here is what scientists said happened beneath the earth’s surface and what to expect in the aftermath:
WHERE DID THE EARTHQUAKE ORIGINATE?
The epicentre was about 26 km east of the Turkish city of Nurdagi at a depth of about 18 km on the East Anatolian Fault. The quake radiated towards the northeast, bringing devastation to central Turkey and Syria.
During the 20th century, the East Anatolian Fault yielded little major seismic activity. “If we were going simply by (major) earthquakes that were recorded by seismometers, it would look more or less blank,” said Roger Musson, an honorary research associate at the British Geological Survey.
Only three earthquakes have registered above 6.0 on the Richter Scale since 1970 in the area, according to the U.S. Geological Survey. But in 1822, a 7.0 quake hit the region, killing an estimated 20,000 people.
HOW BAD WAS THIS EARTHQUAKE?
On average, there are fewer than 20 quakes over 7.0 magnitude in any year, making Monday’s event severe.
Compared with the 6.2 earthquake that hit central Italy in 2016 and killed some 300 people, the Turkey-Syria earthquake released 250 times as much energy, according to Joanna Faure Walker, head of the University College London Institute for Risk and Disaster Reduction.
Only two of the deadliest earthquakes from 2013 to 2022 were of the same magnitude as Monday’s quake.
WHY WAS IT SO SEVERE?
The East Anatolian Fault is a strike-slip fault.
In those, solid rock plates are pushing up against each other across a vertical fault line, building stress until one finally slips in a horizontal motion, releasing a tremendous amount of strain that can trigger an earthquake.
The San Andreas Fault in California is perhaps the world’s most famous strike-slip fault, with scientists warning that a catastrophic quake is long overdue.
The initial rupture for the Turkey-Syria earthquake kicked off at a relatively shallow depth.
“The shaking at the ground surface will have been more severe than for a deeper earthquake of the same magnitude at source,” David Rothery, a planetary geoscientist at the Open University in Britain, said.
WHAT KIND OF AFTERSHOCKS CAN BE EXPECTED?
Eleven minutes after the initial quake, the region was hit by a 6.7-magnitude aftershock. A 7.5-magnitude quake came hours later, followed by another 6.0 spasm in the afternoon.
“What we are seeing now is the activity is spreading to neighbouring faults,” said Musson. “We expect seismicity to continue for a while.”
After the deadly 1822 event, aftershocks carried on into the following year.
WHAT MIGHT THE FINAL DEATH TOLL BE?
Earthquakes of similar magnitudes in populated areas have killed thousands of people. Nepal’s 7.8-magnitude earthquake in 2015 claimed nearly 9,000 lives.
“It’s not going to be good,” said Musson. “It will be in the thousands, and could be in the tens of thousands.”
Cold winter weather, he added, means that people trapped under rubble have less chance at survival.
(Reporting by Gloria Dickie; Editing by Andrew Cawthorne)
Is ‘Quiet Thriving’ the New Workplace Trend We Should All Be Channeling?
Fiona Ward – February 6, 2023
If quiet quitting was your workplace buzzword for 2022, then maybe this year’s more optimistic trend—quiet thriving—might just be the positive outlook you need.
By the end of last year, it seemed we were all quiet quitting something, be it our relationships or our jobs. That is, doing the bare minimum in a situation that you don’t believe is serving you or rewarding you in the way you feel you deserve. But while it’s a tempting thought to mentally check out of your job, it can actually have a pretty negative effect on your mood and may even make you feel even more unfulfilled at work. So, introducing the antithesis to quiet quitting: quiet thriving.
Coined by psychotherapist Lelsey Alderman in an article for The Washington Post, the term quiet thriving means actively making changes to your work day in order to shift your mental state and help you feel more engaged in your job.
As neuroscientist and success coach Laura Ellera tells Glamour UK, it isn’t really in our nature to do the bare minimum at work. “Let’s be honest, it’s not always possible to just up and quit our jobs when they are causing us distress, even though we might want to,” she says. “We can choose to settle into just getting by and practicing quiet quitting, but this in the long run will not be best for your mental health.”
It’s the idea of staying in a job you’re fundamentally unhappy in.
She continues, “We are built to thrive as human beings—we are naturally inquisitive and even if we say we’re happy just doing the bare minimum until something better comes along, deep down we feel that lack of purpose. We notice the clock ticking as our careers seem to drift by us. We are nagged by that feeling that there’s got to be more to life than this.
“Even if you could leave that role, you may not find the fulfillment you crave if you haven’t worked on yourself first. No job alone will give us that deep down satisfaction that we all desire. We want to make a difference. We need to be appreciated. There is a drive to reach our full potential, whether we care to admit it to ourselves or not. So quiet quitting, while it may feel like sticking two up to the establishment, is actually doing the same right back at you.”
For Ellera, quiet thriving allows us to take back control of our well-being at work—and it involves two elements: “The mental switch that we need to work through in order to see our career from a different, more positive angle, and the physical actions we take in order to shape the reality of the role into one that makes us excited to go to work again.”
Here’s how you can try quiet thriving for yourself….
Take back control.
“A great place to start is to think about which parts of your job frustrate you and which parts light you up,” says Ellera. “Really get clear on the different aspects of your role and what they mean to you. Then take the parts that frustrate you and ask yourself honestly, Which parts of this do I have control over? Which parts do I have some influence over? And which parts are completely out of my control?
“If you believe your boss is an overbearing fool, you have no control over how they behave, but you do have control over how you react to their behavior. So go through each of the points (good and bad) and mark ‘control,’ ‘influence,’ or ‘no control’. It’s then down to you to take the parts that light you up and you have control over, and to work out a plan to incorporate more of that into your every day.”
Ellera suggests, “Look at the parts that frustrate you but you have control over, and work out how you can get less of that in your day. Once you’ve worked on these, go onto the things that you have influence over and do the same. Then consciously agree to let go of the things you have no control over. But know that even with these, you always have control over how you choose to react to them. And it is a choice.”
Learn to soothe your nervous system.
“When we get stressed, we lose full access to parts of our brain, as the body is focusing on more imminent threats (previously the hungry lion, now the looming deadline or the angry looking boss heading your way). When our body is in this threat mode, we also lose the ability to communicate properly and build connections with others, both of which are imperative for our workplace success and mental well-being,“ Ellera says.
“So to step out of this threat mode, we need to learn to soothe our nervous system, and we can do this by starting to become more aware of how our body is feeling in the moment. Are you breathing deeply, are your shoulders and jaw relaxed, are you feeling calm? Or are you taking short breaths in the top of your chest, feeling like you’re about to explode?
“Set a reminder on your phone to repeat every hour, and when it goes off, just take notice,” she instructs. “Become aware of what’s happening internally. Allow yourself the grace of taking three long, deep breaths in, exhaling each as slowly as you can through pursed lips, imagining you’re breathing out through a straw. This allows your nervous system to calm and means that your body can function fully and your brain can work optimally—because you can’t thrive in your job if your body is stuck in threat mode.”
It takes a lot of energy for our body to function properly, and a lot of the time, we are taking more out of it than we are replenishing. This means we end up in an energy deficit; that’s when we feel sluggish, sleepy or downright exhausted.
“One thing that can help us to feel rejuvenated is to connect with people who make us feel safe,” says Ellera. “People who feel good to be around. This is when we can co-regulate our nervous systems—we move into step with other people’s breathing and heart-rate rhythm when we are relaxed with them. This can give us more energy and motivation in our workday. The key to this is making sure these relationships are built with growth in mind, so not hanging around with the group that spend their time complaining about work or their boss.
“You also need to be able to trust that person,” she says, ”because although the best thing for your nervous system is another human being, the worst thing for your nervous system is also another human being if they make you feel unsafe in any way shape or form. So connecting with your colleagues has greater benefits than just feeling good. It can actually help to regulate your entire body, give you more energy, and therefore allow you to thrive in your career.”
Have a break.
According to Ellera, there’s no harm in taking time to reset—it may even help with your productivity (depending on what you do, of course).
“We were not built to concentrate for 12 hours straight a day,” she says. “Studies have found that we can only really concentrate on a task for around an hour at a time before our brain starts to wander. So as you push on throughout the day, you’re actually getting less and less efficient at your work and are more and more likely to make mistakes. So take a break.”
One tactic Ellera suggests: “Split the day up into chunks where you can, and make sure you get up, move, and have a break. I get my clients to use the Pomodoro technique, where they set a timer (I use 25 minute intervals) and focus solely on one task at a time; when the timer goes off, they can either reset it and continue for another 25 minutes if it’s going well, or get up and have a break. This will make you so much more productive and helps you to get more done in your day. The breaks allow your brain to rest and your concentration to reset. And if you add a mini reward for getting that task done, such as a five-minute walk outside, or a coffee from the office cafe, your body will anticipate the reward and hit you with a shot of dopamine, the feel good hormone, making you more likely to do it again.”
Most offices have eight-hour workdays—how many of those hours are we really supposed to be working? We asked a productivity expert, a psychologist, a labor journalist, and a boss.
Prioritize your health and sleep.
“If you’re struggling with finding the love for your work, this isn’t going to be improved by crawling into the office late, tired, and with a hangover,” says Ellera. “Our mental health depends on our brain health, and when we don’t look after our brain, this is when everything seems to get harder.
“And this makes appreciating your role and working toward a better career path more difficult if you’re feeling generally rubbish.” she points out. “So ensure you’re starting your working day from the best place possible. Your brain thrives when it is nourished with the right nutrients, hydrated with water and rested with seven to nine hours of sleep. All the stuff that is common sense, but often not common practice. So take stock of where your health is right now. Because that has a direct impact on your brain health. And that has a direct impact on how you are going to be showing up at work and in your life in general.”
Be proactive.
While not every role out there has the wiggle room to change dramatically, there are always more ways to mold the role than we believe, according to Ellera.
“Since you’ve already highlighted the things that light you up over the things that drain you, it’s now up to you to shape your role into something that works for both you and your employer. It’s much more beneficial for an employer to have happy, motivated employees than it is to rigidly stick to a job description without taking into account the human doing the role. And businesses are becoming more open to this way of thinking,” Ellera says.
“Whilst taking a sledgehammer to your role and changing it completely might not go down so well, highlighting areas of opportunity to your boss, and explaining why and how they could work for you and the company, can help you to take back control of your career. Becoming known as the go-to for the area you thrive in will not only make you happier in your role, but also makes you a valued member of the team and increases your potential in the company.”
These are the 7 most common long COVID symptoms, new study finds
Linda Carroll – February 6, 2023
mixetto
Despite the plethora of symptoms reported by patients with long COVID, a new study points to just seven that are unique to the illness. However, some long COVID researchers and doctors who’ve treated the disease believe this list is far from comprehensive.
The goal of the study was to look for long COVID symptoms that appear or persist more than a month after the initial infection and are distinct from symptoms of other common respiratory viruses, such as the flu or common cold. To do so, researchers used Cerner Real-World Data, a database containing information extracted from the electronic medical records from 122 health systems in the U.S.
They analyzed data from electronic health records of more than 17,000 patients diagnosed with COVID before April 14, 2022; more than 17,000 patients diagnosed with a different respiratory virus between March 1, 2020, and April 1, 2021; and 15,694 people with no virus diagnosis but who sought health care between 2020 and 2022.
Researchers concluded that some symptoms typically associated with long COVID do not appear more often after a COVID infection than they do with other respiratory viruses, according to the report published in Open Forum Infectious Diseases.
Compared to other viral respiratory illnesses, long COVID was most strongly associated with:
Heart palpitations (fast beating, fluttering or pounding)
Hair loss
Fatigue
Chest pain
Dyspnea (difficulty breathing)
Joint pain
Obesity in the postinfectious period
The hope is that this research will help patients and their doctors more easily recognize long COVID, study co-author Dr. Adnan Qureshi, neurologist at University of Missouri Health Care, tells TODAY.com. The research may help “health care providers know what they should be screening for,” Qureshi adds.
The surge in long COVID cases caught the health care system by surprise, Qureshi says.
“We thought once you survived the acute infection, then everything would be over,” he explains. “Now that survival has improved a lot, it’s quite apparent that this is not a one-time thing for many.”
“There has been a dramatic shift in disability and loss of productivity on a nationwide scale that is quite out of line with what we expected,” Qureshi adds. “The whole health care system has to gear up to meet that existing demand.”
Qureshi admits that the list of seven symptoms might not be the last word on the topic. “This is a work in progress,” he says. “It’s possible that some of the symptoms did not come out as significant in this analysis.”
Dr. Lawrence Purpura, director of Columbia University Irving Medical Center’s long COVID clinic, tells TODAY.com that the main strength of the new study is the number of patients it includes. But he adds that the study missed some of the cardinal symptoms of long COVID, aka post-COVID syndrome — most likely due to the underlying data. Chief among theses symptoms are:
Brain fog
Disabling fatigue
Dysfunction of the autonomic nervous system, which controls subconscious bodily functions, such as breathing, heart rate and blood pressure
The dysfunction of the autonomic nervous system explains why some patients’ heart rates skyrocket after climbing two or three steps, and that symptom may be what the authors of the new study are listing as heart palpitations, Purpura says.
But there are numerous issues with using electronic medical records to make conclusions about long COVID, Purpura explains.
First, the study depends on doctors knowing enough about long COVID to correctly enter the diagnostic billing code for the illness into the patient’s record, he says. Moreover, many patients with mild cases of COVID aren’t tested for COVID, so it’s wrong to assume that the 15,694 patients in the control group never had COVID.
As a result of the state of testing during the time period covered by the study, people with severe illness were most likely to be tested for COVID by a health care provider.
“In my clinic, I am seeing a lot of patients who were fully vaccinated and who have gone on to develop a prolonged case of long COVID, despite having had a mild case of COVID,” Purpura says. “My concern is that by missing some of the key characteristics of long COVID, we’d be doing patients a disservice.”
David Putrino, Ph.D., director of rehabilitation innovation for the Mount Sinai Health System, tells TODAY.com that, right now, electronic medical record-based studies of long COVID shouldn’t be seen “as anything other than general hypothesis-generating pieces of work.”
“We need to stop treating these studies as the be all and end all of science just because of the large (number of patients) and despite serious methodological flaws,” he adds.
Like Purpura, Putrino has found that the majority of people with persistent long COVID symptoms had a mild case of COVID, so they were unlikely to have positive test results in their medical records.
He adds that one of the big symptoms missed by the new study is “exertional malaise,” the crushing fatigue some patients experience after minor physical exertion. “This is a cardinal symptom of long COVID, and it’s been left out.”
Unfortunately, many health care providers don’t know how to treat this symptom, Putrino says. They think that patients are out of shape from being sick and just need to work up to a higher level of fitness, he adds.
“The reason they are not able to walk a block isn’t because they spent two weeks on the couch recovering from COVID,” Putrino explains. “They are experiencing this because they have inflamed blood vessels, persistent virus still rampaging through the body,” and malfunctioning mitochondria, the power plants of the cells that provide energy to essentially keep the lights on.
“If you try to exert yourself, it’s like someone poisoned you,” Putrino says. “You crash for weeks on end.”
Doctor sitting at desk and writing a prescription for her patient (demaerre via Getty Images)
HOT FLASHES, SLEEPLESSNESS, PAIN DURING SEX: FOR SOME OF MENOPAUSE’S WORST SYMPTOMS, THERE’S AN ESTABLISHED TREATMENT. WHY AREN’T MORE WOMEN OFFERED IT?
For the past two or three years, many of my friends, women mostly in their early 50s, have found themselves in an unexpected state of suffering. The cause of their suffering was something they had in common, but that did not make it easier for them to figure out what to do about it, even though they knew it was coming: It was menopause.
The symptoms they experienced were varied and intrusive. Some lost hours of sleep every night, disruptions that chipped away at their mood, their energy, the vast resources of good will that it takes to parent and to partner. One friend endured weeklong stretches of menstrual bleeding so heavy that she had to miss work. Another friend was plagued by as many as 10 hot flashes a day; a third was so troubled by her flights of anger, their intensity new to her, that she sat her 12-year-old son down to explain that she was not feeling right — that there was this thing called menopause and that she was going through it. Another felt a pervasive dryness in her skin, her nails, her throat, even her eyes — as if she were slowly calcifying.
Then last year, I reached the same state of transition. Technically, it is known as perimenopause, the biologically chaotic phase leading up to a woman’s last period, when her reproductive cycle makes its final, faltering runs. The shift, which lasts, on average, four years, typically starts when women reach their late 40s, the point at which the egg-producing sacs of the ovaries start to plummet in number. In response, some hormones — among them estrogen and progesterone — spike and dip erratically, their usual signaling systems failing. During this time, a woman’s period may be much heavier or lighter than usual. As levels of estrogen, a crucial chemical messenger, trend downward, women are at higher risk for severe depressive symptoms. Bone loss accelerates. In women who have a genetic risk for Alzheimer’s disease, the first plaques are thought to form in the brain during this period. Women often gain weight quickly, or see it shift to their middles, as the body fights to hold onto the estrogen that abdominal fat cells produce. The body is in a temporary state of adjustment, even reinvention, like a machine that once ran on gas trying to adjust to solar power, challenged to find workarounds.
I knew I was in perimenopause because my period disappeared for months at a time, only to return with no explanation. In the weeks leading up to each period, I experienced abdominal discomfort so extreme that I went for an ultrasound to make sure I didn’t have some ever-growing cyst. At times, hot flashes woke me at night, forcing me straight into the kinds of anxious thoughts that take on ferocious life in the early hours of morning. Even more distressing was the hard turn my memory took for the worse: I was forever blanking on something I said as soon as I’d said it, chronically groping for words or names — a development apparent enough that people close to me commented on it. I was haunted by a conversation I had with a writer I admired, someone who quit relatively young. At a small party, I asked her why. “Menopause,” she told me without hesitation. “I couldn’t think of the words.”
My friends’ reports of their recent doctors’ visits suggested that there was no obvious recourse for these symptoms. When one friend mentioned that she was waking once nightly because of hot flashes, her gynecologist waved it off as hardly worth discussing. A colleague of mine seeking relief from hot flashes was prescribed bee-pollen extract, which she dutifully took with no result. Another friend who expressed concerns about a lower libido and vaginal dryness could tell that her gynecologist was uncomfortable talking about both. (“I thought, hey, aren’t you a vagina doctor?” she told me. “I use that thing for sex!”)
Their doctors’ responses prompted me to contemplate a thought experiment, one that is not exactly original but is nevertheless striking. Imagine that some significant portion of the male population started regularly waking in the middle of the night drenched in sweat, a problem that endured for several years. Imagine that those men stumbled to work, exhausted, their morale low, frequently tearing off their jackets or hoodies during meetings and excusing themselves to gulp for air by a window. Imagine that many of them suddenly found sex to be painful, that they were newly prone to urinary-tract infections, with their penises becoming dry and irritable, even showing signs of what their doctors called “atrophy.” Imagine that many of their doctors had received little to no training on how to manage these symptoms — and when the subject arose, sometimes reassured their patients that this process was natural, as if that should be consolation enough.
Now imagine that there was a treatment for all these symptoms that doctors often overlooked. The scenario seems unlikely, and yet it’s a depressingly accurate picture of menopausal care for women. There is a treatment, hardly obscure, known as menopausal hormone therapy, that eases hot flashes and sleep disruption and possibly depression and aching joints. It decreases the risk of diabetes and protects against osteoporosis. It also helps prevent and treat menopausal genitourinary syndrome, a collection of symptoms, including urinary-tract infections and pain during sex, that affects nearly half of postmenopausal women.
Menopausal hormone therapy was once the most commonly prescribed treatment in the United States. In the late 1990s, some 15 million women a year were receiving a prescription for it. But in 2002, a single study, its design imperfect, found links between hormone therapy and elevated health risks for women of all ages. Panic set in; in one year, the number of prescriptions plummeted. Hormone therapy carries risks, to be sure, as do many medications that people take to relieve serious discomfort, but dozens of studies since 2002 have provided reassurance that for women under 60 whose hot flashes are troubling them, the benefits of taking hormones outweigh the risks. The treatment’s reputation, however, has never fully recovered, and the consequences have been wide-reaching. It is painful to contemplate the sheer number of indignities unnecessarily endured over the past 20 years: the embarrassing flights to the bathroom, the loss of precious sleep, the promotions that seemed no longer in reach, the changing of all those drenched sheets in the early morning, the depression that fell like a dark curtain over so many women’s days.
About 85 percent of women experience menopausal symptoms. Rebecca Thurston, a professor of psychiatry at the University of Pittsburgh who studies menopause, believes that, in general, menopausal women have been underserved — an oversight that she considers one of the great blind spots of medicine. “It suggests that we have a high cultural tolerance for women’s suffering,” Thurston says. “It’s not regarded as important.”
Even hormone therapy, the single best option that is available to women, has a history that reflects the medical culture’s challenges in keeping up with science; it also represents a lost opportunity to improve women’s lives.
“EVERY WOMAN HAS the right — indeed the duty — to counteract the chemical castration that befalls her during her middle years,” the gynecologist Robert Wilson wrote in 1966. The U.S. Food and Drug Administration approved the first hormone-therapy drug in 1942, but Wilson’s blockbuster book, “Feminine Forever,” can be considered a kind of historical landmark — the start of a vexed relationship for women and hormone therapy. The book was bold for its time, in that it recognized sexual pleasure as a priority for women. But it also displayed a frank contempt for aging women’s bodies and pitched hormones in the service of men’s desires: Women on hormones would be “more generous” sexually and “easier to live with.” They would even be less likely to cheat. Within a decade of the book’s publication, Premarin — a mix of estrogens derived from the urine of pregnant horses — was the fifth-most-prescribed drug in the United States. (Decades later, it was revealed that Wilson received funding from the pharmaceutical company that sold Premarin.)
In 1975, alarming research halted the rise of the drug’s popularity. Menopausal women who took estrogen had a significantly increased risk of endometrial cancer. Prescriptions dropped, but researchers soon realized that they could all but eliminate the increased risk by prescribing progesterone, a hormone that inhibits the growth of cells in the uterus lining. The number of women taking hormones started rising once again, and continued rising over the next two decades, especially as increasing numbers of doctors came to believe that estrogen protected women from cardiovascular disease. Women’s heart health was known to be superior to men’s until they hit menopause, at which point their risk for cardiovascular disease quickly skyrocketed to meet that of age-matched men. In 1991, an observational study of 48,000 postmenopausal nurses found that those who took hormones had a 50 percent lower risk of heart disease than those who did not. The same year, an advisory committee suggested to the F.D.A. that “virtually all” menopausal women might be candidates for hormone therapy. “When I started out, I had a slide that said estrogen should be in the water,” recalls Hadine Joffe, a psychiatry professor at Harvard Medical School who studies menopause and mood disorders. “We thought it was like fluoride.”
Feminist perspectives on hormone therapy varied. Some perceived it as a way for women to control their own bodies; others saw it as an unnecessary medicalization of a natural process, a superfluous product designed to keep women sexually available and conventionally attractive. For many, the issue lay with its safety: Hormone therapy had already been aggressively marketed to women in the 1960s without sufficient research, and many women’s health advocates believed that history was repeating itself. The research supporting its health benefits came from observational studies, which meant that the subjects were not randomly assigned to the drug or a placebo. That made it difficult to know if healthier women were choosing hormones or if hormones were making women healthier. Women’s health advocates, with the support of the feminist congresswoman Patricia Schroeder, called on the National Institutes of Health to run long-term, randomized, controlled trials to determine, once and for all, whether hormones improved women’s cardiovascular health.
In 1991, Bernadine Healy, the first woman to serve as director of the N.I.H., started the Women’s Health Initiative, which remains the largest randomized clinical trial in history to involve only women, studying health outcomes for 160,000 postmenopausal women, some of them over the course of 15 years. Costs for just one aspect of its research, the hormone trial, would eventually run to $260 million. The hormone trial was expected to last about eight years, but in June 2002, word started spreading that one arm of the trial — in which women were given a combination of estrogen and progestin, a synthetic form of progesterone — had been stopped prematurely. Nanette Santoro, a reproductive endocrinologist who had high hopes for hormones’ benefit on heart health, told me she was so anxious to know why the study was halted that she could barely sleep. “I kept waking my husband up in the middle of the night to say, ‘What do you think?’” she recalled. Alas, her husband, an optometrist, could scarcely illuminate the situation.
Santoro did not have to wait long. On July 9, the Women’s Health Initiative’s steering committee organized a major news conference in the ballroom of the National Press Club in Washington to announce both the halting of the study and its findings, a week before the results would be publicly available for doctors to read and interpret. Jaques Rossouw, an epidemiologist who was the acting director of the W.H.I., told the gathered press that the study had found both adverse effects and benefits of hormone therapy, but that “the adverse effects outweigh and outnumber the benefits.” The trial, Rossouw said, did not find that taking hormones protected women from heart disease, as many had hoped; on the contrary, it found that hormone therapy carried a small but statistically significant increased risk of cardiac events, strokes and clots — as well as an increased risk of breast cancer. He described the increased risk of breast cancer as “very small,” or more precisely: “less than a tenth of 1 percent per year” for an individual woman.
What happened next was an exercise in poor communication that would have profound repercussions for decades to come. Over the next several weeks, researchers and news anchors presented the data in a way that caused panic. On the “Today” show, Ann Curry interviewed Sylvia Wassertheil-Smoller, an epidemiologist who was one of the chief investigators for the W.H.I. “What made it ethically impossible to continue the study?” Curry asked her. Wassertheil-Smoller responded, “Well, in the interest of safety, we found there was an excess risk of breast cancer.” Curry rattled off some startling numbers: “And to be very specific here, you actually found that heart disease, the risk increased by 29 percent. The risks of strokes increased by 41 percent. It doubled the risk of blood clots. Invasive breast cancer risk increased by 26 percent.”
All of those statistics were accurate, but for a lay audience, they were difficult to interpret and inevitably sounded more alarming than was appropriate. The increase in the risk of breast cancer, for example, could also be presented this way: A woman’s risk of having breast cancer between the ages of 50 and 60 is around 2.33 percent. Increasing that risk by 26 percent would mean elevating it to 2.94 percent. (Smoking, by contrast, increases cancer risk by 2,600 percent.) Another way to think about it is that for every 10,000 women who take hormones, an additional eight will develop breast cancer. Avrum Bluming, a co-author of the 2018 book “Estrogen Matters,” emphasized the importance of putting that risk and others in context. “There is a reported risk of pulmonary embolism among postmenopausal women taking estrogen,” Bluming says. “But what is ‘risk’? The risk of embolism is similar to the risk of being on oral contraceptives or being pregnant.”
The study itself was designed with what would come to be seen as a major flaw. W.H.I. researchers wanted to be able to measure health outcomes — how many women ended up having strokes, heart attacks or cancer — but those ailments may not show up until women are in their 70s or 80s. The study was scheduled to run for only 8½ years. So they weighted the participants toward women who were already 60 or older. That choice meant that women in their 50s, who tended to be healthier and have more menopausal symptoms, were underrepresented in the study. At the news conference, Rossouw started out by saying that the findings had “broad applicability,” emphasizing that the trial found no difference in risk by age. It would be years before researchers appreciated just how wrong that was.
The “Today” segment was just one of several media moments that triggered an onslaught of panicked phone calls from women to their doctors. Mary Jane Minkin, a practicing OB-GYN and a clinical professor at Yale School of Medicine, told me she was apoplectic with frustration; she couldn’t reassure her patients, if reassurance was even in order (she came to think it was), because the findings were not yet publicly available. “I remember where I was when John Kennedy was shot,” Minkin says. “I remember where I was on 9/11. And I remember where I was when the W.H.I. findings came out. I got more calls that day than I’ve ever gotten before or since in my life.” She believes she spoke to at least 50 patients on the day of the “Today” interview, but she also knows that countless other patients did not bother to call, simply quitting their hormone therapy overnight.
Within six months, insurance claims for hormone therapy had dropped by 30 percent, and by 2009, they were down by more than 70 percent. JoAnn Manson, chief of the division of preventive medicine at Brigham and Women’s Hospital and one of the chief investigators in the study, described the fallout as “the most dramatic sea change in clinical medicine that I have ever seen.” Newsweek characterized the response as “near panic.” The message that took hold then, and has persisted ever since, was a warped understanding of the research that became a cudgel of a warning: Hormone therapy is dangerous for women.
THE FULL PICTURE of hormone therapy is now known to be far more nuanced and reassuring. When patients tell Stephanie Faubion, the director of the Mayo Clinic Center for Women’s Health, that they’ve heard that hormones are dangerous, she has a fairly consistent response. “I sigh,” Faubion told me. She knows she has some serious clarifying to do.
Faubion, who is also the medical director of the North American Menopause Society (NAMS), an association of menopause specialists, says the first question patients usually ask her is about breast-cancer risk. She explains that in the W.H.I. trial, women who were given a combination of estrogen and progestin saw an increased risk emerge only after five years on hormones — and even after 20 years, the mortality rate of women who took those hormones was no higher than that of the control group. (Some researchers have hope that new formulations of hormone therapy will lessen the risk of breast cancer. One major observational study published last year suggested so, but that research is not conclusive.)
The biggest takeaway from the last two decades of research is that age matters: For women who go through early menopause, before age 45, hormone therapy is recommended because they’re at greater risk for osteoporosis if they don’t receive hormones up until the typical age of menopause. For healthy women in their 50s, life-threatening events like clots or stroke are rare, and so the increased risks from hormone therapy are also quite low. When Manson, along with Rossouw, did a reanalysis of the W.H.I. findings, she found that women under 60 in the trial had no elevated risk of heart disease.
The findings, however, did reveal greater risks for women who start hormone therapy after age 60. Manson’s analyses found that women had a small elevated risk of coronary heart disease if they started taking hormones after age 60 and a significant elevated risk if they started after age 70. It was possible, researchers have hypothesized, that hormones may be most effective within a certain window, perpetuating the well-being of systems that are still healthy but accelerating damage in those already in decline. (No research has yet followed women who start in their 50s and stay on continuously into their 60s.)
Researchers also now have a better appreciation of the benefits of hormone therapy. Even at the time that the W.H.I. findings were released, the data showed at least one clear improvement resulting from hormone therapy: Women had 24 percent fewer fractures. Since then, other positive results have emerged. The incidence of diabetes, for instance, was found to be 20 percent lower in women who took hormones, compared with those who took a placebo. In the W.H.I. trial, women who had hysterectomies — 30 percent of American women by age 60 — were given estrogen alone because they did not need progesterone to protect them from endometrial cancer, and that group had lower rates of heart disease and breast cancer than the placebo group. “Nonetheless,” Bluming and his co-author, Carol Tavris, write in “Estrogen Matters,” “we have yet to see an N.I.H. press conference convened to reassure women of the benefits of estrogen.” Anything short of that, they argue, allows misrepresentations and fears to persist.
Positive reports about hormone therapy for women in their 50s started emerging as early as 2003, and they have never really slowed. But the revelations have come in a trickle, with no one story gaining the kind of exposure or momentum of the W.H.I. news conference. In 2016, Manson tried to rectify the problem in an article for The New England Journal of Medicine, issuing a clear course correction of the W.H.I. findings as they pertained to women in their 40s and 50s. Since she published that paper, she feels, attitudes have changed, but too slowly. Manson frequently speaks to the press, and as the years passed — and more data accumulated that suggested the risks were not as alarming as they were first presented — you can almost track her increasing frustration in her public comments. “Women who would be appropriate candidates are being denied hormone therapy for the treatment of their symptoms,” she told me in a recent interview. She was dismayed that some doctors were not offering relief to women in their 50s on the basis of a study whose average subject age was 63 — and in which the risk assessments were largely driven by women in their 70s. “We’re talking about literally tens of thousands of clinicians who are reluctant to prescribe hormones.”
Even with new information, doctors still find themselves in a difficult position. If they rely on the W.H.I., they have the benefit of a gold-standard trial, but one that focused on mostly older women and relied on higher doses and different formulations of hormones from those most often prescribed today. New formulations more closely mimic the natural hormones in a woman’s body. There are also new methods of delivery: Taking hormones via transdermal patch, rather than a pill, allows the medication to bypass the liver, which seems to eliminate the risk of clots. But the studies supporting the safety of newer options are observational; they have not been studied in long-term, randomized, controlled trials.
The NAMS guidelines emphasize that doctors should make hormone-therapy recommendations based on the personal health history and risk factors of each patient. Many women under 60, or within 10 years of menopause, already have increased baseline risks for chronic disease, because they are already trying to manage their obesity, hypertension, diabetes or high cholesterol. Even so, Faubion says that “there are few women who have absolute contraindications,” meaning that for them, hormones would be off the table. At highest risk from hormone use are women who have already had a heart attack, breast cancer or a stroke or a blood clot, or women with a cluster of significant health problems. “For everyone else,” Faubion says, “the decision has to do with the severity of symptoms as well as personal preferences and level of risk tolerance.”
For high-risk women, other sources of relief exist: The selective serotonin reuptake inhibitor paroxetine is approved for the relief of hot flashes, although it is not as effective as hormone therapy. Cognitive-behavioral therapy has also been shown to help women with how much hot flashes bother them. Doctors who treat menopause are waiting for the F.D.A.’s review of a drug up for approval this month: a nonhormonal drug that would target the complex of neurons thought to be involved in triggering hot flashes.
Conversations about the risks and benefits of these various treatments often require more time than the usual 15-minute slot that health insurance will typically reimburse for a routine medical visit. “If I weren’t my own chair, I would be called to task for not doing stuff that would make more money, like delivering babies and I.V.F.,” says Santoro, now the department chair of obstetrics and gynecology at the University of Colorado School of Medicine, who frequently takes on complex cases of menopausal women. “Family medicine generally doesn’t want to deal with this, because who wants to have a 45-minute-long conversation with somebody about the risks and benefits of hormone therapy? Because it’s nuanced and complicated.” Some of those conversations entail explaining that hormones are not a cure-all. “When women come in and tell me they’re taking hormones for anti-aging or general prevention, or because they have some vague sense it’ll return them to their premenopausal self — and they’re not even having hot flashes — I say, ‘Hormone therapy is not a fountain of youth and shouldn’t be used for that purpose,’” Faubion says.
Too many doctors are not equipped to parse these intricate pros and cons, even if they wanted to. Medical schools, in response to the W.H.I., were quick to abandon menopausal education. “There was no treatment considered safe and effective, so they decided there was nothing to teach,” says Minkin, the Yale OB-GYN. About half of all practicing gynecologists are under 50, which means that they started their residencies after the publication of the W.H.I. trial and might never have received meaningful education about menopause. “When my younger partners see patients with menopausal symptoms, they refer them to me,” says Audrey Buxbaum, a 60-year-old gynecologist with a practice in New York. Buxbaum, like many doctors over 50, prescribed menopausal hormone therapy before the W.H.I. and never stopped.
Education on a stage of life that affects half the world’s population is still wildly overlooked at medical schools. A 2017 survey sent to residents across the country found that 20 percent of them had not heard a single lecture on the subject of menopause, and a third of the respondents said they would not prescribe hormone therapy to a symptomatic woman, even if she had no clear medical conditions that would elevate the risk of doing so. “I was quizzing my daughter a few years ago when she was studying for the board exams, and whoever writes the board questions, the answer is never, ‘Give them hormones,’” Santoro says. In recent years, there has been some progress: The University of Pennsylvania has established a menopause clinic, and Johns Hopkins now offers a two-year curriculum on the subject to its medical students. But the field of gynecology will, most likely for decades to come, be populated by many doctors who left medical school unprepared to offer guidance to menopausal women who need their help.
I DIDN’T KNOW all of this when I went to see my gynecologist. I knew only what my friends had told me, and that hormone therapy was an option. The meeting was only my second with this gynecologist, a woman who struck me as chic, professional and in a bit of a hurry, which was to be expected, as she is part of a large health care group — the kind that makes you think you’d rather die from whatever’s ailing you than try to navigate its phone tree one more time. Something about the quick pace of the meeting — the not-so-frequent eye contact — made me hesitate before bringing up my concerns: They felt whiny, even inappropriate. But I forged on. I was having hot flashes, I told her — not constantly, but enough that it was bothering me. I had other concerns, but since memory issues were troubling me the most, I brought that up next. “But that could also just be normal aging,” she said. She paused and fixed a doubtful gaze in my direction. “We only prescribe hormones for significant symptoms,” she told me. I felt rebuffed, startled by how quickly the conversation seemed to have ended, and I was second-guessing myself. Were my symptoms, after all, “significant”? By whose definition?
The NAMS guidelines suggest that the benefits of hormone therapy outweigh the risks for women under 60 who have “bothersome” hot flashes and no contraindications. When I left my doctor’s office (without a prescription), I spent a lot of time thinking about whether my symptoms were troubling me enough to take on any additional risk, no matter how small. On the one hand, I was at a healthy weight and active, at relatively low risk for cardiovascular disease; on the other hand, because of family history and other factors, I was at higher risk for breast cancer than many of my same-age peers. I felt caught between the promises and, yes, risks of hormone therapy, the remaining gaps in our knowledge and my own aversion, common if illogical, to embarking on a new and indefinitely lasting medical regimen.
Menopause could represent a time when women feel maximum control of our bodies, free at last from the risk of being forced to carry an unwanted pregnancy. And yet for many women, menopause becomes a new struggle to control our bodies, not because of legislation or religion but because of a lack of knowledge on our part, and also on the part of our doctors. Menopause presents not just a new stage of life but also a state of confusion. At a time when we have the right to feel seasoned, women are thrust into the role of newbie, or worse, medical detective, in charge of solving our own problems.
Even the most resourceful women I know, the kind of people you call when you desperately need something done fast and well, described themselves as “baffled” by this stage of their lives. A recent national poll found that 35 percent of menopausal women reported that they had experienced four or more symptoms, but only 44 percent said they had discussed their symptoms with a doctor. Women often feel awkward initiating those conversations, and they may not even identify their symptoms as menopausal. “Menopause has the worst P.R. campaign in the history of the universe, because it’s not just hot flashes and night sweats,” says Rachel Rubin, a sexual-health expert and assistant clinical professor in urology at Georgetown University. “How many times do I get a 56-year-old woman who comes to me, who says, Oh, yeah, I don’t have hot flashes and night sweats, but I have depression and osteoporosis and low libido and pain with sex? These can all be menopausal symptoms.” In an ideal world, Rubin says, more gynecologists, internists and urologists would run through a list of hormonal symptoms with their middle-aged patients rather than waiting to see if those women have the knowledge and wherewithal to bring them up on their own.
The W.H.I. trial measured the most severe, life-threatening outcomes: breast cancer, heart disease, stroke and clots, among others. But for a woman who is steadily losing hair, who has joint pain, who suddenly realizes her very smell has changed (and not for the better) or who is depressed or exhausted — for many of those women, the net benefits of taking hormones, of experiencing an improved quality of life day to day, may be worth facing down whatever incremental risks hormone therapy entails, even after age 60. Even for women like me, whose symptoms are not as drastic but whose risks are low, hormones can make sense. “I’m not saying every woman needs hormones,” Rubin says, “but I’m a big believer in your body, your choice.”
Conversations about menopause lack, among so many other things, the language to help us make these choices. Some women sail blissfully into motherhood, but there is a term for the extreme anxiety and depression that other women endure following delivery: postpartum depression. Some women menstruate every month without major upheaval; others experience mood changes that disrupt their daily functioning, suffering what we call premenstrual syndrome (PMS), or in more serious cases, premenstrual dysphoric disorder. A significant portion of women suffer no symptoms whatsoever as they sail into menopause. Others suffer near-systemic breakdowns, with brain fog, recurring hot flashes and exhaustion. Others feel different enough to know they don’t like what they feel, but they are hardly incapacitated. Menopause — that baggy term — is too big, too overdetermined, generating a confusion that makes it especially hard to talk about.
NO SYMPTOM is more closely associated with menopause than the hot flash, a phenomenon that’s often reduced to a comedic trope — the middle-aged woman furiously waving a fan at her face and throwing ice cubes down her shirt. Seventy to 80 percent of women have hot flashes, yet they are nearly as mysterious to researchers as they are to the women experiencing them — a reflection of just how much we still have to learn about the biology of menopause. Scientists are now trying to figure out whether hot flashes are merely a symptom or whether they trigger other changes in the body.
Strangely, the searing heat a woman feels roaring within is not reflected in any significant rise in her core body temperature. Hot flashes originate in the hypothalamus, an area of the brain rich in estrogen receptors that is both crucial in the reproductive cycle and also functions as a thermostat. Deprived of estrogen, its thermostat now wonky, the hypothalamus is more likely to misread small increases in core body temperature as too hot, triggering a rush of sweat and widespread dilation of the blood vessels in an attempt to cool the body. This also drives up the temperature on the skin. Some women experience these misfirings once a day, others 10 or more, with each one lasting anywhere from seconds to five minutes. On average, women experience them for seven to 10 years.
What hot flashes might mean for a woman’s health is one of the main questions that Rebecca Thurston, the director of the Women’s Biobehavioral Health Laboratory at the University of Pittsburgh, has been trying to answer. Thurston helped lead a study that followed a diverse cohort of 3,000 women over 22 years and found that about 25 percent of them were what she called superflashers: Their hot flashes started long before their periods became irregular, and the women continued to experience them for as many as 14 years, upending the idea that, for most women, hot flashes are an irritating but short-lived inconvenience. Of the five racial and ethnic groups Thurston studied, Black women were found to experience the most hot flashes, to experience them as the most bothersome and to endure them the longest. In addition to race, low socioeconomic status was associated with the duration of women’s hot flashes, suggesting that the conditions of life, even years later, can affect a body’s management of menopause. Women who experienced childhood abuse were 70 percent more likely to report night sweats and hot flashes.
Might those symptoms also signal harm beyond the impact on a woman’s quality of life? In 2016, Thurston published a study in the journal Stroke showing that women who had more hot flashes — at least four a day — tended to have more signs of cardiovascular disease. The link was even stronger than the association between cardiovascular risk and obesity, or cardiovascular risk and high blood pressure. “We don’t know if it’s causal,” Thurston cautions, “or in which direction. We need more research.” There might even be some women for whom the hot flashes do accelerate physical harm and others not, Thurston told me. At a minimum, she says, reports of severe and frequent hot flashes should cue doctors to look more closely at a woman’s cardiac health.
As Thurston was trying to determine the effects of hot flashes on vascular health, Pauline Maki, a professor of psychiatry at the University of Illinois at Chicago, was establishing associations between hot flashes and mild cognitive changes during menopause. Maki had already found a clear correlation between the number of a woman’s hot flashes and her memory performance. Maki and Thurston wondered if they would be able to detect some physical representation of that association in the brain. They embarked on research, published last October, that found a strong correlation between the number of hot flashes a woman has during sleep and signs of damage to the tiny vessels of the brain. At a lab in Pittsburgh, which has one the most powerful M.R.I. machines in the world, Thurston showed me an image of a brain with tiny lesions represented as white dots, ghostlike absences on the scan. Both their number and placement, she said, were different in women with high numbers of hot flashes. But whether the hot flashes were causing the damage or the changes in the cerebral vessels were causing the hot flashes, she could not say.
About 20 percent of women experience cognitive decline during perimenopause and in the first years after menopause, mostly in the realm of verbal learning, the acquisition and synthesis of new information. But the mechanisms of that decline are varied. As estrogen levels drop, the region of the brain associated with verbal learning is thought to recruit others to support its functioning. It’s possible that this period of transition, when the brain is forming new pathways, accounts for the cognitive dip that some women experience. For most of them, it’s short-lived, a temporary neurological confusion. A woman’s gray matter — the cells that process information — also seems to shrink in volume before stabilizing in most women, according to Lisa Mosconi, an associate professor of neurology at Weill Cornell Medicine and director of its Women’s Brain Initiative. She compares the process the brain undergoes during those years of transition to a kind of “remodeling.” But the tiny brain lesions that Thurston and Maki detected don’t resolve — they remain, contributing incrementally, over many years, to an increased risk of cognitive decline and dementia.
In the past 15 years, four randomized, controlled trials found that taking estrogen had no effect on cognitive performance. But those four studies, Maki points out, did not look specifically at women with moderate to severe hot flashes. She believes that might be the key factor: Treat the hot flashes with estrogen, Maki theorizes, and researchers might see an improvement in cognitive health. In one small trial Maki conducted of about 36 women, all of whom had moderate to severe hot flashes, half of the group received a kind of anesthesia procedure that reduced their hot flashes, and the other half received a placebo treatment. She measured the cognitive function of both groups before the treatment and then three months after and found that as hot flashes improved, memory improved. The trial was small but “hypothesis generating,” she says.
Even adjusting for greater longevity in women, Alzheimer’s disease is more frequent in women than men, one of many brain-health discrepancies that have led researchers to wonder about the role that estrogen — and possibly hormone therapy — might play in the pathways of cognitive decline. But the research on hormone therapy and Alzheimer’s disease has proved inconclusive so far.
Whatever research exists on hormones and the brain focuses on postmenopausal women, which means it’s impossible to know, for now, whether perimenopausal women could conceivably benefit from taking estrogen and progesterone during the temporary dip in their cognitive function. “There hasn’t been a single randomized trial of hormone therapy for women in perimenopause,” Maki says. “Egregious, right?”
What’s also unclear, Thurston says, is how the various phenomena of cognitive change during menopause — the temporary setbacks that resolve, the progress toward Alzheimer’s in women with high genetic risk and the onset of those markers of small-vessel brain disease — interact or reflect on one another. “We haven’t followed women long enough to know,” says Thurston, who believes that menopause care begins and ends with one crucial dictum: “We need more research.”
IN THE information void, a vast menopausal-wellness industry has developed, flush with products that Faubion dismisses as mostly “lotions and potions.” But a new crop of companies has also come to market to provide F.D.A.-approved treatments, including hormone therapy. Midi Health offers virtual face-to-face access to menopause-trained doctors and nurse practitioners who can prescribe hormones that some insurances will cover; other sites, like Evernow and Alloy, sell prescriptions directly to the patient. (Maki serves on the medical advisory boards of both Midi and Alloy.)
On the Alloy website, a woman answers a series of questions about her symptoms, family and medical history, and the company’s algorithm recommends a prescription (or doesn’t). A prescribing doctor reviews the case and answers questions by text or phone, and if the woman decides to complete the order, she has access to that prescribing doctor by text for as long as the prescription is active.
Alloy holds online support groups where women, clearly of varying socioeconomic backgrounds, often vent — about how hard it was for them to find relief, how much they are still suffering or how traumatized they still are by the lack of compassion and concern they encountered when seeking help for distressing symptoms. On one call in July, a middle-aged woman described severe vaginal dryness. “When I was walking or trying just to exercise, I would be in such agony,” she said. “It’s painful just to move.” She was trying to buy vaginal estradiol cream, an extremely low-risk treatment for genitourinary syndrome; she said there was a shortage of it in her small town. Until she stumbled on Alloy, she’d been relying on antibacterial creams to soothe the pain she felt.
The space was clearly a no-judgment zone, a place where women could talk about how they personally felt about the risks and benefits of taking hormones. At one meeting, a woman said that she’d been on hormone therapy, which she said “changed my life” during perimenopause, but that she and her sisters both had worrying mammograms at the same time. Her sister was diagnosed with breast cancer and had her lymph nodes removed; the woman on the call was diagnosed with atypical hyperplasia, which is not cancer but is considered a precursor that puts a woman at high risk. The NAMS guidelines do not indicate that hormone therapy is contraindicated for a woman at high risk of breast cancer, leaving it up to the woman and her practitioner to decide. “My new OB-GYN and my cancer doc won’t put me on hormones,” the woman said. She bought them from Alloy instead. “So I’m kind of under the radar.”
No one at the meeting questioned the woman’s decision to go against the advice of two doctors. I mentioned the case to Faubion. “It sounds to me like she felt she wasn’t being heard by her doctors and had to go somewhere else,” she said. Faubion told me that in certain circumstances, higher-risk women who are fully informed of the risks but suffer terrible symptoms might reasonably make the decision to opt for hormones. But, she said, those decisions require nuanced, thoughtful conversations with health care professionals, and she wondered whether Alloy and other online providers were set up to allow for them. Anne Fulenwider, one of Alloy’s founders, said the patient in the support group had not disclosed her full medical history when seeking a prescription. After that came to light, an Alloy doctor reached out to her to have a more informed follow-up conversation about the risks and benefits of hormone therapy.
As I weighed my own options, I sometimes asked the doctors I interviewed outright for their advice. For women in perimenopause, who are still at risk of pregnancy, I learned, a low-dose birth control can “even things out,” suppressing key parts of the reproductive system and supplying a steadier dose of hormones. Another alternative is an intrauterine device (IUD) to provide birth control, along with a low-dose estrogen patch, which is less potent than even a low-dose birth-control pill and is therefore thought to be safer. “Too much equipment,” I told Rachel Rubin, the sexual-health expert, when she suggested it. “This is why I don’t ski.” I found myself thinking often about an insight that Santoro says she offers her patients (especially those under 60 and in good health): If you’re having any symptoms, how can you weigh the risks and benefits if you haven’t experienced the extent of the benefits?
In November, I started on a low-dose birth-control pill. I am convinced — and those close to me are convinced — that my brain is more glitch-free. I have no hot flashes. Most surprising to me (and perhaps the main reason for that improvement in cognition): My sleep improved. I had not even mentioned my poor quality of sleep to my gynecologist, given the length of our discussion, but I had also assumed that it was a result of stress, age and a sweet but snoring husband. Only once I took the hormones did I appreciate that my regular 2 a.m. wakings, too, were most likely a symptom of perimenopause. The pill was an easy-enough experiment, but it carried a potentially higher risk of clots than the IUD and patch; now convinced that the effort of an IUD is worth it, I resolved to make that switch as soon as I could get an appointment.
How many women are doing some version of what I did, unsure of or explaining away menopausal symptoms, apologizing for complaining about discomforts they’re not sure are “significant,” quietly allowing the conversation to move on when they meet with their gynecologists or internists or family-care doctors? And yet … my more smoothly functioning brain goes round and round, wondering, worrying, waiting for more high-quality research. Maybe in the next decade, when my personal risks start escalating, we’ll know more; all I can hope is that it confirms the current trend toward research that reassures. The science is continuing. We wait for progress, and hope it is as inevitable as aging itself.
Colorado River crisis is so bad, lakes Mead and Powell are unlikely to refill in our lifetimes
Rong-Gong Lin II, Ian James – February 5, 2023
Boaters are dwarfed by a white bathtub ring around Lake Mead. (Luis Sinco/Los Angeles Times)
The snowpack in the Sierra Nevada is the deepest it’s been in decades, but those storms that were a boon for Northern California won’t make much of a dent in the long-term water shortage for the Colorado River Basin — an essential source of supplies for Southern California.
In fact, the recent storms haven’t changed a view shared by many Southern California water managers: Don’t expect lakes Mead and Powell, the nation’s largest reservoirs, to fill up again anytime soon.
“To think that these things would ever refill requires some kind of leap of faith that I, for one, don’t have,” said Brad Udall, a water and climate scientist at Colorado State University.
Lake Mead, located on the Arizona-Nevada border and held back by Hoover Dam, filled in the 1980s and 1990s. In 2000, it was nearly full and lapping at the spillway gates. But the megadrought over the last 23 years — the most severe in centuries — has worsened the water deficit and left Lake Mead about 70% empty.
Even with this winter’s above-average snowpack in the Rocky Mountains, water officials and scientists say everyone in the Colorado River Basin will need to plan for low reservoir levels for years to come. And some say they think the river’s major reservoirs probably won’t refill in our lifetimes.
“They’re not going to refill. The only reason they filled the first time is because there wasn’t demand for the water. In the 1950s, ’60s, ’70s and ’80s, there was no Central Arizona Project, there was no Southern Nevada Water Authority, there was not nearly as much use in the Upper [Colorado River] Basin,” said Bill Hasencamp, manager of Colorado River resources for the Metropolitan Water District of Southern California. “So the water use was low. So that filled up storage.”
Demand for Colorado River water picked up in the late 1990s and early 2000s. The Central Arizona Project, a 336-mile-long water delivery system, brings water from the Colorado River to Arizona’s most populous counties and wasn’t completed until the 1990s. The Southern Nevada Water Authority was created in 1991.
Arizona began starting to take its full apportionment of river water in the late 1990s, and Nevada in the early 2000s. California continues using the single largest share of the river.
“Now the water use is maxed out. Every state is taking too much, and we have to cut back. And so there’s just not enough. You would need wet year after wet year, after wet year after wet year, after wet year. Even then, because the demand is so high, it still wouldn’t fill,” Hasencamp said in an interview.
Climate change has dramatically altered the river. In the last 23 years, as rising temperatures have intensified the drought, the river’s flow has declined about 20%.
Scientists have found that roughly half the decline in the river’s flow has been caused by higher temperatures, and that climate change is driving the aridification of the Southwest. With global warming, average temperatures across the upper watershed — where most of the river’s flow originates — have risen about 3 degrees since 1970.
Research has shown that for each additional 1 degree Celsius (1.8 degrees Fahrenheit), the river’s average flow is likely to decrease about 9%.
In multiple studies, scientists have estimated that by the middle of this century, the average flow of the river could decline by 30% or 40% below the average during the past century.
“The last 23 years are the best lessons we have right now, and they should scare the pants off of people,” said Udall, who has been a co-author of research showing how warming is sapping the river’s flows.
Based on the low levels of Lake Mead and Lake Powell, Udall said, he would estimate that refilling the reservoirs would take roughly six consecutive extremely wet years, with water flows similar to those in 2011.
“We’d need six years like that to refill this system, in a row, based on current operating rules,” Udall said. “And I just don’t see that even being remotely possible.”
The Colorado River Basin very well could get a few wet years, he said.
“We might even get a wet decade. But, boy, the long-term warming and drying trend seems super clear to me,” Udall said. “And a bet on anything other than that seems like water management malpractice, that we have got to plan for something that looks like a worst-case future.”
The Colorado River supplies water to seven states, tribal nations and Mexico. The states are under pressure from the federal government to agree on cuts to prevent reservoirs from dropping to dangerously low levels.
California and the six other states are at odds over how to make the cuts, and have submitted separate proposals to the federal government, with some disagreements centering on the legal system that governs how the river is managed.
In a 2008 study, scientists Tim Barnett and David Pierce examined the likely flow declines with climate change and estimated there was a 50% chance the usable water supply in Lake Mead and Lake Powell would be gone by 2021. They titled their study “When Will Lake Mead Go Dry?” In research published in 2009, they wrote that based on projections with climate change or even the long-term average flows, “currently scheduled future water deliveries from the Colorado River are not sustainable.”
“Climate change is reducing the flow into the Colorado River system, so the agreements are divvying up more water than exists,” said Pierce, a climate scientist at Scripps Institution of Oceanography. “This drop in reservoir levels is happening because we are abiding by agreements that do not account for changes in water inflow into the system due to climate change.”
There is always the chance of a few extremely wet years with the potential to refill reservoirs, Pierce said.
“It’s just that in the coming decades that likelihood decreases. Our work has estimated that the chance of the reservoirs refilling decreases from about 75% today to about 10% by 2060 if no changes in [water] delivery schedules are made,” Pierce said. “We should be planning for the situation where the hotter temperatures decrease the river flow in the future.”
The capacity of lakes Mead and Powell is gargantuan compared with the capacity of California’s two largest reservoirs, Shasta Lake and Lake Oroville. Lake Mead can store more than 27 million acre-feet of water, and Lake Powell 25 million acre-feet. By contrast, Shasta Lake can hold about 4.6 million acre-feet, and Lake Oroville 3.5 million acre-feet.
The Colorado River supplies, on average, about 25% of the water supplies in coastal Southern California, while the region also gets water from Northern California through the State Water Project, and other sources.
California’s Sierra Nevada snowpack is now about 200% of average at this point in the season, while the snowpack in the Upper Colorado River Basin so far stands at about 140% of the median over the last 30 years.
The bigger snowpack could help the Colorado’s reservoir levels this year somewhat. How much won’t be clear for a few months.
“Absolutely this snow is welcomed. The cold weather is welcome. The real question will be in the spring,” Hasencamp said.
In recent years, hot, dry conditions have led to reduced flows in the river. “That’s what’s been the killer the last few years, is a hot dry spring has taken the snow that’s been there, and it doesn’t make it to the reservoirs,” Hasencamp said.
Daniel Swain, a UCLA climate scientist, said an exceptionally wet decade might someday change things.
“But the problem is, it doesn’t just have to be wetter than average, it would have to be dramatically wetter than the long-term average,” Swain said. And for many years.
Scientists say higher temperatures effectively make the atmosphere “thirstier,” causing more moisture to evaporate off the landscape. Vegetation also takes up more water as temperatures rise, leaving less runoff flowing in streams.
“There is no question that there will be an ongoing downward trend in inflows, but extreme high events are also more likely to occur in the context of climate change, according to the U.S. National Climate Assessment,” said Kathy Jacobs, director of the University of Arizona’s Center for Climate Adaptation Science and Solutions.
Jacobs noted that researchers project atmospheric rivers will become more intense with rising temperatures, and scientists expect more intense extreme storms and periodic flooding.
“I strongly suspect that the dams on the Colorado will be needed for flood control in the future as well as for water supply,” Jacobs said.
As for the future, Jacobs said a great deal depends on whether greenhouse gas emissions are reduced “to net zero in the near term.”
There are workable ways of managing reduced water supplies from the river, she said. “The longer we wait to build more flexible future management schemes, the harder it will be.”
It’s everywhere: Sea-level rise’s surprising reach damaging more than East Coast shoreline
Kelly Powers and Dinah Voyles Pulver – February 5, 2023
Sections of 2,200 feet of geotextile tubes installed in 2019 behind 13 private lots on Ponte Vedra Beach have been uncovered by erosion from a recent storm.
A walk down this 6-mile stretch of Florida beach might feel different than others.
Some things are the same. Rolling waves reach into smooth sheets, polishing the beach. Seaweed and shells tumble and settle, tumble and settle.
Look to the land, and the view is unexpected. Dunes have been carved into jagged cliffs. Strange canvas tubing pokes out of eroding sand mounds.
Keep walking and the view changes again. Newly imported plants grip a rebuilt dune, the result of an expensive human project.
Ponte Vedra Beach is just one place that provides a firsthand view of all the problems storm surge and high tides and sea-level rise bring in with them.
Seawalls jut from the sand, blamed by some for additional erosion elsewhere. Residents installed over 2,000 feet of geotextile tubing along the beaten dunes, with mixed results.
Meanwhile, their homes peer over a sand cliff’s edge.
“People are trying to beat Mother Nature,” said Nancy Condron, who built a home on this beach with her husband in 2008. “And what they really need to do is move their structures back and have a natural dune.”
Condron has been vocal in her opinions, having built west of the state’s coastal construction limits, but debates persist.
“It’s depressing.”
Sea-level rise is deeper than tides, more than the beach
This slice of Florida nearly captures sea-level rise in its full scope.
The sea advances on St. Johns County with a deadly combination of naturally higher tides, empowered storms and saltwater intrusion. It will impact generations of businesses, deeply historic neighborhoods, freshwater public supply wells, sparkling new subdivisions and oceanfront mansions alike.
But accelerated sea-level rise isn’t just a beachfront problem.
From threatened heritage to salty forests, oyster farms and inland flooding, voices across the region show this threat and its mitigation are far more complex than higher tides.
The rising sea reaches places you would not expect.
One tide gauge in the nation broke its record for high-tide flood days over the past year.
It was far inland, just outside Delaware City along Delaware Bay and about 20 miles from Wilmington, Delaware.
Places up and down the entire East Coast are menaced by sea-level rise’s impacts compounding the force of tides and storms: centuries of Black history, generations of businesses on Philadelphia’s Schuylkill River, headstones in colonial New England cemeteries, millennia of indigenous Florida heritage.
One of the oldest Black American communities feels current turning against them
She raised all the air conditioners 18 inches.
Lincolnville Museum and Cultural Center’s executive director Gayle Phillips in St. Augustine doesn’t have the budget to approach large mitigation projects, so she makes hands-on fixes. “We didn’t want to invest in AC units that were just going to be subjected to flooding,” Phillips said.
The effort came after Hurricane Matthew. Across much of Lincolnville’s east and south sides, flooding occurs during high tide and heavy rain.
Phillips is no stranger to taking her shoes off to get to work.
The museum, cradled by its historically Black neighborhood of Lincolnville, is devoted in part to celebrating the history of those taken involuntarily over this ocean centuries ago.
St. Augustine is the oldest continuously occupied European settlement in the country. Tourists come for its history, architecture and the white quartz sand of its beaches.
Now St. Augustine is fighting the sea to preserve indigenous artifacts, colonial Spanish antiquity and modern Black history. Newly freed slaves established the now-historic district of Lincolnville inside a city already more than 450 years old.
In 1964, Lincolnville hosted a famed Martin Luther King Jr. sit-in. Not only would King be arrested in St. Augustine that June, he would be in the city to learn the Civil Rights Act had passed.
History is baked into these 45 blocks of southwest peninsula.
The Lincolnville museum finds itself in competition with historical settlements, buildings and landmarks all around it for precious funds to preserve its own piece of heritage — in a place where there’s almost as much history as there is water.
Water’s winning.
But Lincolnville is just one neighborhood, and competition for funding is already steep. Phillips is not alone in her concern that the history she safeguards will be sacrificed for something more popular.
She said the Lincolnville museum cannot afford drainage improvements to its parking lot right now. It could be hard to imagine visitors taking off their shoes, wading through frequent flood waters, to reach her doors.
Lincolnville didn’t rank as highly as the Castillo de San Marcos fort, among other sites, in a recent city assessment of archaeological value. Historic tourism is worth $2.9 billion.
Pennsylvania brewpub fights back against storms, tides and sea-level rise
Up and down East Coast states, impact reaches well inland of the high tide line.
Mike Rose watched the damage unfold under a clear sky.
After the raging storm commanded attention all night, Pennsylvania officials continued to warn of a Schuylkill River surge near Philadelphia. More than 17 feet was expected by 8 a.m. It crested just short of that.
Rose watched from an off-site monitor as the cameras streamed the destruction until the power went out. The 66-year-old is used to occasional flooding, but this was different.
He returned to nearly three feet of mud.
Gelled between toppled equipment, saturated walls and debris, brown slime coated the guts of his restaurant. Massive brewpub tanks had been lifted and dropped. Remains blocked any path to Manayunk Brewing Company’s back patio, typically overlooking a quietly flowing river, several yards below.
“Did I think I was going to open up this time? I didn’t think so,” Rose recalled, perched at the bar. “I said: ‘I don’t know if I want to do this. I’m stripped. I’m just stripped of strength.”
Remnants of Hurricane Ida brought a Schuylkill River surge that near-completely engulfed Manayunk Brewing Restaurant and Bar on Sept. 2, 2021, in northwest Philadelphia. The brewpub, having made hundreds of its own craft beers since 1996, reopened after six months of repairs as a restaurant and bar.Hurricane Irene, Hurricane Isaias, an unnamed flash flood in 2014, Agnes from 1972 — various high-water lines climb the wall in Manayunk Brewing Restaurant and Bar, in Philadelphia, on July 22, 2020. Black arrows mark each floodwater peak.
He swiped through photos on his phone. Employees shoveled mud. Ruined wiring ripped from the walls. Pieces of kitchen equipment were shoved in a heap against the iron street gate.
From the Chesapeake to Massachusetts bays, Ida brought surges several feet above typical high tide levels.
Rising seas can spell problems for inland communities. High tides and strengthened storm surges push water higher in nearby rivers during extreme storms, and into floodplains.
Rivers across Pennsylvania and New Jersey broke record levels.
Higher tides also push back on rivers, preventing flow back into the sea. Meanwhile, fresh water from extreme rainfall can start stacking up.
If it can’t drain into watersheds, it will find new routes.
Charged by climate change, stronger storms expose weaknesses
“Hurricanes have multiple elements or drivers or mechanisms here,” said Ning Lin, associate professor of civil and environmental engineering with Princeton University. “Sea-level rise is one piece.
“Looking at the joint probability between rainfall and surge, with sea-level rise, we found that extreme joint hazards can become much more frequent in our future climate.”
The strongest drivers for this, Lin said, are more intense rainfall — as a warming planet draws more water into the atmosphere, contributing to heavier storms — and a rising sea.
She said more research is needed to model for these impacts, together. Ida already exposed mid-Atlantic infrastructure shortcomings.
Rose may feel too busy for all the science. He has his third restaurant to run.
Nearly $2 million in Ida repairs later, the brewpub reopened in February. Repairing beer tanks proved too expensive. “We’re not making our own beer anymore,” Rose said. “That’s devastating to us.”
Kitchen equipment sits on wheels. Newly polished floors replace any carpeting. Electric panels were moved to the second floor.
Over Rose’s shoulder, small signs climb the gray bricks. Markers for Hurricane Irene, Hurricane Isaias, an unnamed flash flood in 2014, Agnes in 1972 — the various high-water lines stretch back to the building’s time as a wool mill. Black arrows mark floodwater peaks.
The edge of Ida’s small, white sign meets the ceiling. And it points up.
Underground, another waterline snakes its way inland.
Saltwater seeps underground into critical freshwater wetlands
Only the notes of historians remain to tell the story of the Pamlico people.
They lived along the Albemarle and Pamlico sounds for thousands of years, on the now-North Carolina coast, gliding dugout canoes through wetland forest threaded with teeming creeks and rivers.
This is “TaTaku” — where land and sea meet the sky — but the Pamlico vanished within 150 years of European settlers’ arrival. Men, women and children were decimated by smallpox and absorbed into other tribes.
Scientists fear the Albemarle-Pamlico Peninsula could follow a similar path. Freshwater wetland forests and shrubby evergreen bogs could be decimated by rising seas and absorbed by advancing coastal marsh.
Wildlife refuges protect more than 450,000 acres, hosting migratory birds, rare pocosin peat bogs and the sole wild population of red wolves in the nation. Today, fewer than two dozen remain.
With no escape, the cedars, pines and pocosin bogs starve under an onslaught of rising water. On this peninsula, Atlantic white cedars have virtually disappeared.
Sea water presses forward into the estuary, past Outer Banks barrier islands. Salinity levels creep higher, pushing into groundwater supplies and washing overland during high tides and storm surges.
These rolling pulses already arrive more often.
Once the sea water arrives, trapped by roads and other changes in elevation, it can stay for weeks, or even months — saturating the roots of the trees.
Forests could be completely overtaken, said Elliott White Jr., assistant professor at Stanford University. Satellite photos show the landward march. A dense, brown fringe “gets thicker and thicker year after year.”
If the losses documented over 25 years continue without widespread restoration, White said, the wetland forests could disappear by the end of this century.
The insidious flow of salts below ground also threatens freshwater wells and agriculture across the region. Farmers on the peninsula, who raise corn, soybeans, wheat, potatoes and cotton, have seen salt in their fields, said Rebekah Martin, Coastal NC National Wildlife Refuges Complex project leader.
“Ghost forests” can grow almost slowly enough to miss. Yet these dying woods appear from Maine to Miami, bending back along the Gulf of Mexico.
Stripped of their leaves and bark, trees become gaunt skeletons. Gradually forests and bogs give way to more salt-tolerant thickets.
“I’ve seen palm tree ghost forests in Florida and red spruce ghost forests in Canada,” said Matt Kirwan, associate professor with Virginia Institute of Marine Science. “They all share a similar origin.”
A group of University of South Florida researchers concluded the Big Bend’s coastal forest is dying at “an unprecedented rate.”
Hurricane Sandy left a ghost forest of white cedar in New Jersey.
In the Chesapeake Bay region, more than 80,000 acres of forest have turned to marsh in the last 150 years. That number could increase fivefold by 2100, Kirwan predicts.
New corridors would have to be considered for wildlife to retreat, Martin said. And more people and places could be exposed to intensifying storms typically buffered by marsh.
On the Albemarle-Pamlico Peninsula, once-vital forests could be lost to history.
Unwitting oysters part of a plan to fortify shorelines
Rolling between Scott Budden’s fingers, a baby oyster resembles a grain of sand. Its tiny shell, still translucent in the gray morning, is already the perfect shape.
Its life with Budden begins here on Kent Island, Maryland. Farmers must tailor the crop’s controlled life cycle with the whims of changing waters, rising tides and shifting salinity.
After outgrowing land tanks, having savored algae and phytoplankton, the adolescent oyster will eventually move north to the Chester River. Waves will crash through hundreds of similar surface floats, transferring energy to the bundled mollusks lining several acres.
The oyster will return to Eastern Bay to finish. The water is saltier down here.
Scott Budden with a handful of seed oysters on July 26, 2022, destined for oyster reefs. In term of broader restoration, Joseph Gordon of Pew says the Chesapeake Bay is already the most massive shellfish restoration project in the world, central to a life system stretching from Maine to Florida. “It’s the beating heart of the Atlantic coast,” he said.Oyster tattoos on the arm of Scott Budden on July 26, 2022. He escaped his Washington, D.C., finance job in 2012 to come work on Kent Island.
Today, his prize crop joins a growing list of natural tools to fight against the very waters that foster it. Experts say even these oysters raised for a plate can also help fortify shorelines, like millions once did on their own.
“Growing the shellfish aquaculture industry can benefit the entire ecosystem,” said Joseph Gordon, U.S. East Coast project director with Pew Charitable Trusts. His group co-sponsored an initiative to buy millions of oysters from farmers like Budden, who were lacking the usual restaurant demand, and re-establish them in the bay.
The initiative’s reach extended to shellfish growers up the mid-Atlantic and New England, following an idea that has established itself to grow much like the oysters themselves: Mitigating climate change can mimic the natural world.
What’s a living shoreline?
One farm offers a payoff Budden doesn’t often consider.
On a stretch of coast, he notices an exposed beach has slowly washed away. But the same erosion, near Eastern Neck Island, Maryland, isn’t seen on his side.
“I’ve noticed there’s some dampening effect,” said the 36-year-old. “Basically, as waves come through, the energy is transferred to the floats, the floats then transfer that energy to the oyster. Which, actually, makes a better oyster.”
His casual observations echo the experts and other projects. Mitigations have been moving “from gray to green” to combat the effects of rising sea.
“For a long time, when we needed to stop erosion along the shoreline, we put in a hard structure,” said Molly Mitchell, a research assistant professor with the Virginia Institute of Marine Science. Think bulkheads, riprap, seawalls.
“They don’t provide good habitat for animals, and they don’t have the other benefits of natural beaches and marshes, like actually reducing wave energy.”
“Living shorelines” — from adding marsh and grass, to building shellfish breakwaters — have been growing in popularity as an alternative to shoreline hardening.
Scott Budden washes a bin by the dock on July 26, 2022. Today, his prize crop joins a growing list of natural tools to help the very waters that foster it. “Adding oysters can even help other interconnected habitats, like salt marsh and underwater seagrass — and together, these can increase the integrity and resilience of the coast by stabilizing shorelines to better withstand storms and storm surge,” said Joseph Gordon, U.S. East Coast project director with Pew Charitable Trusts.
Oyster reefs once thrived on Eastern shores, before humans decimated populations in the early 1800s. Oysters built on top of one another as others died, creating a solid structure.
“Rocks and seawalls aren’t going to evolve as the water gets steeper,” Mitchell said. “If you use an oyster reef, the oysters will actually grow on it — and the structure will get taller and taller as sea level rises.”
It can’t work everywhere. These solutions take best to systems with more moderate wave energy, like the Chesapeake Bay, or rivers and sounds.
Back at the dock, Budden and his team watch saltwater drizzle through a churning tumbler, cleaning their harvest. Those measuring too small plunk back to the bay below.
His crop has always had a role to play in protecting the coast, but today shoreline communities may need to get more creative.
“We’ve got a couple million market oysters in the water, another three or four million have been put through the nursery this year,” he said. “Still, just a drop in the bucket.”
This article is part of a USA TODAY Network reporting project called “Perilous Course,” a collaborative examination of how people up and down the East Coast are grappling with the climate crisis. Journalists from more than 35 newsrooms from New Hampshire to Florida are speaking with regular people about real-life impacts, digging into the science and investigating government response, or lack of it.